
Get full access with a free account
Benefits of the Coloplast® Professional Educational platform
- Full access to educational content, events and resources
- Track your progress
- Share content with your colleagues
- Share supporting material with your patient
To completely empty the bladder, repositioning is needed, but there is a greater risk of bladder microtrauma when repositioning.1 Both residual urine due to incomplete bladder emptying and microtrauma constitute a risk for UTIs.2
Of the 90% ISC users that reposition their catheter, 78% experience that the urine starts to run again. This means that the bladder is not completely empty at first flow stop.3
Flow stops make complete bladder emptying uncertain and complex:
- Uncertain as flow stops give a false indication of an emptied bladder
- Complex because the user needs to reposition1
The importance of repositioning is also underlined in the EAUN clinical guidance.4
"When urine flow stops, withdraw the catheter very slowly, in centimetre steps. If the urine flow starts again during withdrawal, discontinue withdrawal and wait for the flow to stop before resuming catheter withdrawal"
Why catheter repositioning is necessary / 0.38 min
What are flow stops and how do they occur?
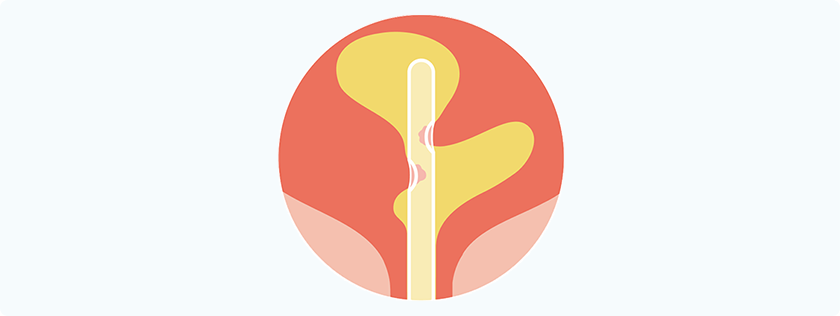
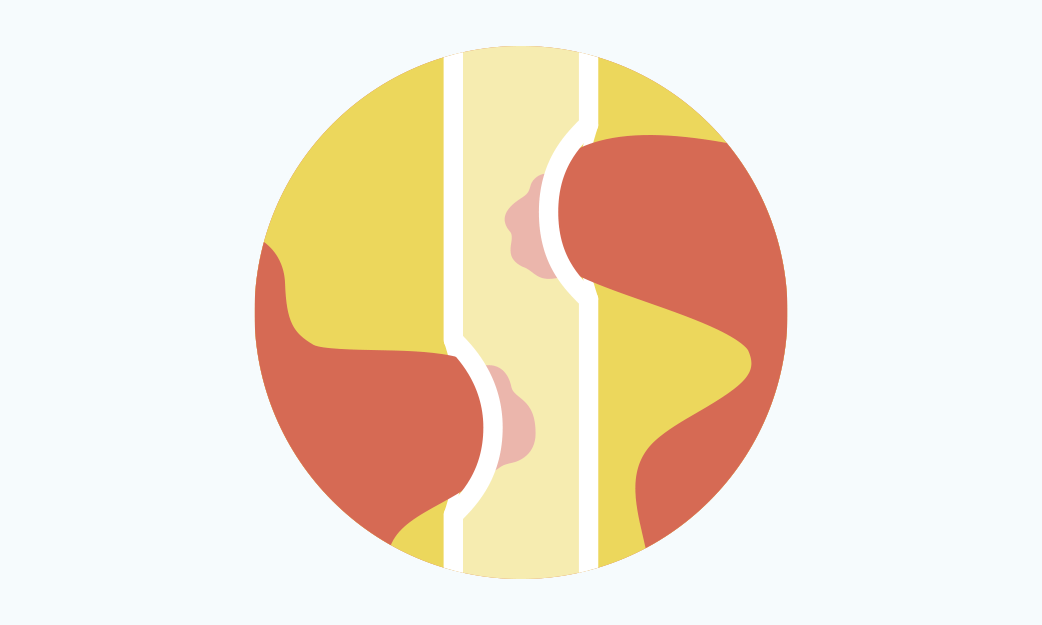
Draining of urine during catheterisation creates negative pressure inside the catheter. This causes the bladder mucosa to get sucked into the eyelets of the catheter, blocking them, leading to a urine flow stop.1
CEC seen from the inside of the catheter, OUH, DK / 1 Minutes
Repositioning of the catheter helps to release the mucosa and continue the draining of urine. Mucosal suction can additionally cause trauma to the bladder wall and compromise the protective layer of the epithelial cells.1 This allows bacteria to attach to and invade the bladder cells, thus increasing the risk of UTI.5,6

Quote
- Kjell Bjørn Rønning